
Post by imperfectgolfer on Aug 12, 2023 13:28:01 GMT -5
I think that Brian Manzella's generic 5-step approach to dealing with a slice problem makes no sense, and I think that the "cure" must be targeted at the particular root cause of the slice swing fault. I will provide some examples of what type of swing fault can cause a sliced shot, and I will show that the "cure" must be precisely targeted at the particular cause of the slice problem.
BM described a basic/generic 5-step program to deal with a slice problem. His first two steps involved his personal "belief" regarding the type of lead hand grip and trail hand grip that a golfer should adopt to avoid slicing the ball, but there is no correlation between a slice swing fault and a particular hand grip pattern. For example, it is commonly believed that a weak lead hand grip can lead to a slice problem, especially if the hands get too far forward at impact, but the true cause of a slice problem under those conditions more likely involves one-or-more factors that interfere with the successful completion of the release of PA#2 and/or PA#3.







BM described a basic/generic 5-step program to deal with a slice problem. His first two steps involved his personal "belief" regarding the type of lead hand grip and trail hand grip that a golfer should adopt to avoid slicing the ball, but there is no correlation between a slice swing fault and a particular hand grip pattern. For example, it is commonly believed that a weak lead hand grip can lead to a slice problem, especially if the hands get too far forward at impact, but the true cause of a slice problem under those conditions more likely involves one-or-more factors that interfere with the successful completion of the release of PA#2 and/or PA#3.
BM's third step was too avoid having the clubshaft pointing left-of-the-target at P4. However, if the clubshaft is still on-plane under those conditions (see Tiger Woods video in the last post) then there should be no reason why it should lead to a slice problem. A "laid-off" clubshaft at P4 can lead to a slice problem because it may make the clubshaft lag too far behind the lead arm in the downswing action resulting in an incomplete release of PA#2 => PA#3.
BM's 4th step was to use his "lagging the sweetspot" technique, which is biomechanically based on the use of the reverse motorcycle move +/- a twistaway maneuver. However, those two maneuvers can only close the clubface by ~30 degrees (relative to the clubhead path) between P4 => P6, and BM stated that the clubface often needs to close by ~110 degrees between P4 => P7. Secondly, if the golfer maintains a bowed lead wrist between P6 => P7, then that will cause an increased degree of forward shaft lean, which is a clubface-opening scenario. I have clearly/repeatedly shown that pro golfers (eg. Jon Rahm and Collin Morikawa), who use the bowed lead wrist technique (that involves use of the reverse motorcyle/twistaway maneuver) with a weak/neutral lead hand grip, actually have to use more lead forearm supination during their PA#3 release action in order to get a square clubface by impact. There is no substitute for a well-executed PA#3 release action that involves a counterclockwise rotation of the lead forearm and the amount of required lead forearm supination during a PA#3 release action is inversely proportional to the strength of the lead hand grip.
BM's 5th step was to recommend that a golfer transition through impact by transitioning very rapidly between a pre-impact PA#3 release action into a post-impact release swivel action, but that is a band-aid approach that will likely cause a high clubface ROC through impact, which is a very timing-dependent swing technique.
I will now provide some examples of swing faults that can cause a slice problem, where the "cure" must be precisely targeted at the swing fault.
Example 1: Straightening right wrist at the P4 position and/or lead hand opening.
Oliver Heuler demonstrates the correct alignment of the RFFW relative to the LFFW at the P4 position in image 1, which requires an extended trail wrist that can correctly align the trail palm parallel to the intact LFFW.
In image 2, OH shows that a straightened trail wrist at P4 can twist the club handle clockwise and cause an open clubface alignment at the P4 position. What OH does not show in his image is the fact that right wrist straightening can also lead to excessive lead wrist cupping at the same time where the clubshaft is simultaneously directed across-the-line. The "cure" is to remedy the incorrect trail wrist alignment at P4.
In image 3, OH shows a scenario where the lead hand does not maintain a firm grip on the club handle, and how the opening finger motion causes the rotating clubshaft to twist the clubface to an open alignment at P4. The "cure" must obviously be targeted at avoiding that particular swing fault.
Example 2: Pelvic slide motion during the downswing.
In this image, OH is demonstrating a scenario where the golfer slides his pelvis too much targetwards in the early downswing and where the outer border of the lead pelvis is well outside the lead foot at impact. That pelvic over-sliding motion can cause a V-shaped hand arc path where the hands get to impact too soon and there is therefore no ability to complete the release of PA#2 by impact resulting in excessive forward shaft lean and an open clubface at impact. The "cure" must obviously be targeted at the root cause of this swing fault.
Example 3: Late club release phenomenon.
In this image, OH is showing the swing fault where a golfer tries to hold a 90 degree clubhead lag angle for too long and where the trail elbow is too far ahead of the trail hip area at P6. That will likely not give the golfer enough time to complete the release of PA#2 => PA#3 resulting in an open clubface at impact. The "cure" must obviously be targeted at the root cause of this swing fault.
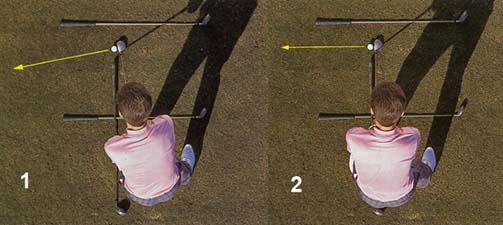
Example 4: "Rock-and-block" swing fault.
OH is demonstrating the "rock-and-block" swing fault.
Image 1 shows an incorrect takeaway action where the hands are pulled inside, but where the clubshaft is kept outside the hands - while avoiding any lead forearm pronation which is needed to rotate the clubshaft onto the swingplane by P2.5 if one uses a RFT takeaway pattern.
Image 2 then shows how the golfer simply lifts up the club during the later backswing while performing a reverse-pivoting motion of the upper torso.
Image 3 then shows how the golfer starts the downswing with a pelvic slide motion (incorporating an early extension motion of the pelvis) in order to correct the reverse-pivoting torso alignment and that causes the head to fall back away from the target as the upper torso tilts away from the target. The golfer's arms are also blocked by the sliding pelvis/mid-torso and they move out to right-field and the clubshaft is pulled forward without the correct performance of the standard U-shaped hand arc path that allows for the efficient release of PA#2/PA#3 by impact. Note the open clubface at impact.
The "cure" must be targeted at the "rock-and-block" swing fault.
Example number 5: Incorrect address alignment of the body/ball.
Image 1 - This golfer has an open foot/shoulder alignment at address with the ball positioned too far forward of the lead foot at address.
Having an open foot/upper torso alignment at address may make it too difficult for an inflexible golfer to perform an efficient clockwise pelvic/upper torso rotation during the backswing and the hands may not get behind the toe line by P4. That will lead to an out-to-in clubhead path during the downswing and when the hands reach their impact position opposite the lead thigh, there will be a scenario of backwards shaft lean, an out-to-in clubhead path and an open clubface (relative to the clubhead path) that will likely lead to a pull-sliced ball flight pattern.
Image 2 shows the "cure" - having a neutral foot/shoulder stance at address and placing the ball inside the lead foot at address.
Placing the ball too far back and closer to the trail foot can also predispose to slicing because there is no time to complete the release of PA#2 => PA#3 by impact - even if the foot/shoulder alignment is correct at address.
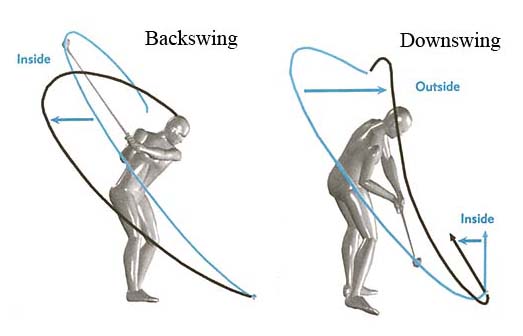
Example number 6: Out-to-in clubhead path due to an OTT move.
This image from the SLAP book shows the correct clubhead path in blue and the incorrect clubhead path in black. Note that the golfer takes the club too much inside between P1 => P4 and then loops the club in an OTT-manner during the early downswing thereby producing an out-to-in clubhead path into impact.
Here are capture images of a golfer manifesting those swing faults.
Image 2 shows the golfer taking the club too much inside.
Image 4 and 5 show him performing an OTT move (also called an "upper body dive" move) that will invariably lead to an out-to-in clubhead path into impact. That will result in a straight pull ball flight if the clubface is square to the clubhead path at impact, but the golfer often tries to rescue the shot by twisting his two arms/hands clockwise as he approaches impact and that will open the clubface (relative to the clubhead path) resulting in a pull-sliced ball flight pattern.
The "cure" must obviously be targeted at correcting all these swing faults, and not be focused on BM's 5-step slice-fixing program!
Example number 7: A disordered kinematic sequence.
In these capture images (image 1 and 2), Russell Heritage shows the correct kinematic sequencing where the pelvis starts the pivot's rotary motion while the upper torso is held back. That allows the golfer to retain his rightwards spinal tilt while he simultaneously performs his trail upper arm adduction motion using a pitch elbow motion of the trail elbow (image 3 and 4). That correct kinematic sequencing leads to an in-to-out clubhead path in the mid-late downswing.
Here are capture images of RH showing an incorrect kinematic sequencing swing fault.
RH shows an incorrect kinematic sequencing where the golfer starts off with an upper torso rotation that throws the lead arm too much outwards while the pelvis remains static from a rotary perspective and does not rotate. Note how the spine/head move targetwards and the spinal tilt becomes leftwards-aligned.
That disordered kinematic sequencing move of the upper body will lead to an out-to-in clubhead path. A golfer will likely try to avoid a straight pull ball flight by twisting the arms/hands clockwise in the later downswing and the clubface will become open (relative to the clubhead path) at impact resulting in a pull-sliced ball flight pattern.
The "cure" must be targeted at correcting the disordered kinematic sequencing problem and not by learning BM's 5-step slice-fixing program!
Example number 8: A lack of coordination between the torso and arm motion during the downswing.
Here is a swing video of Annika Sorenstam performing her ball drill.
Note how the ball (and therefore the two elbows) rotate counterclockwise at the same angular velocity as her rotating torso during the downswing thereby allowing her to keep the ball in front of her rotating chest throughout the downswing and early followthrough, and that represents a synchronised body/arm motion.
Some golfers, in an attempt to generate more swing power, rotate their pelvis far too fast counterclockwise at the start of the downswing, and the pelvis far outraces the upper torso/arms, which lag too far behind. Then, while the pelvis has already rotated counterclockwise to an open alignment by impact, the arms are flung centrifugally out towards right field because they have not rotated inside-left in synchrony with the rotating pelvis. That prevents the proper release of PA#2 => PA#3 and the clubface will likely be far too open at impact leading to a sliced ball flight pattern.
The "cure" is to improve the pivot motion and ensuring that the arms rotate in synchrony with the rotating torso.
Example number 9, 10, 11 ---:
To square the clubface by impact, a golfer who uses a weak-or-neutral lead hand grip, needs to enact a significant amount of lead forearm supination between P6.5 => P7 (representing the release of PA#3) when he performs a TGM swinging action. That requires a relaxed lead forearm that can rotate freely/passively between P6.5 => P7. Any tension in the lead forearm can slow down the passive rotation of the lead forearm that should happen automatically/naturally/ unconsciously leading to the incomplete release of PA#3 => resulting in an open clubface at impact. It also possible for the trail arm's behaviour to result in the incomplete release of PA#3 if the trail arm straightens too fast after P6 and pushes the lead hand/club handle too fast into impact.
Another frequent cause of slicing is to "handle-drag" the club handle towards impact in the late downswing between P6 => P7 without releasing the club. Optimally, the club should start to release between P5.2 - P5.5 and one should avoid "handle-dragging" the club handle into the late downswing phase. The longer the length of the club (eg. driver), the more important it is to release the club sooner so that the sequential release of PA#2 => PA#3 can be efficiently completed before impact.
I could provide some more examples of swing faults that can cause a slice ball flight, but my major purpose of this post is to demonstrate that the correct approach to curing a slice swing fault is to correct the particular swing fault that is causing the "slice" swing fault - rather than to use a generic band-aid approach as advised by BM in that BBG video.
Jeff.








